Providers have begun receiving non-medical additional document requests for claims utilizing the benefit period waiver in response to the COVID-19 public health emergency. These reviewers are being flagged with a “7COVD” code and have primarily been reported under Wisconsin Physician Services (WPS).
These suspended claims may be the result of a billing issue. As such, review the proper guidelines below for how claims involving the waiver for the 60-day wellness period should be billed.
Loneliness and social isolation might seem like conditions that are just “in your head,” but it’s important to recognize the signs and help those who might be impacted.
Types of Loneliness
Emotional
When someone feels the lack of intimate relationships possibly due to the loss of a close partner or friend.
Grief and bereavement support can help provide the tools needed to cherish that relationship and move forward to exploring new ones.
Incorporate activities to honor their loved one (e.g., make a scrap book or photo album).
Social
Lack of satisfying contact with family, friends, neighbors and other community members
Engaging in social activities can help mitigate this one. Encourage the person to dine with others and find activities that inspire them to interact including music, games and other activities hobbies.
If appropriate for the resident(s), incorporate education in the use of smart phones or computers for communication with family and friends.
Collective
Feeling of not being valued by the broader community
Lend a listening ear.
Coordinate a small support group within the community where participants can share their stories, encourage each other and identify opportunities for community involvement.
Facilitate activities that engage the resident and the community in which residents assist the community (e.g., shelling peas for a local farmer).
Existential
The sense that life lacks meaning or purpose
Often older adults feel they have moved from providing for their family to being becoming a burden on them. Help them find a new meaning and purpose such as the following:
Explore small chores in the facility such as:
Helping with a pet therapy animal
Watering or tending plants/gardens
Feeding the birds
Delivering mail or paper
Shower them with lots of appreciation for their contributions – no matter how big or small.
Despite the many adaptations and additional considerations that have been adopted in the battle against COVID-19, healthcare providers in skilled nursing facilities (SNFs) maintain their primary focus of quality patient rehabilitation and care. In the midst of planning and delivering care in a pandemic, some may ask, Does data collection really matter right now? What’s GG got to do with it? The answers are Yes and everything!
CMS has indicated the value of data collection of our patient’s functional abilities (i.e. Section GG) by signaling it as a key comparison of quality across post-acute settings, an indicator of resource use impacting reimbursement, and critical to guiding patient-centered care planning. Although CMS stated exceptions and extensions were granted because data collection may be greatly impacted by the response to COVID-19, beginning July 1, SNFs are expected to report their quality data to meet the SNF QRP requirements for the third quarter of 2020. (Download CMS’ SNF QRP Tip Sheet)
Knowing this data eventually will be publicly posted, the question now becomes Does it reflect our exhausting efforts to deliver care during this public health emergency? That answer is yet to be determined, but it is never too late for a review and refresh of Section GG content as well as considerations for coding and patient identification in the current environment.
Accuracy of Section GG coding depends not only upon the healthcare professional’s familiarity with the objective scales, but also with each item’s definition, intent and parameters for coding. For example, walking items may be completed within separate sessions. A single walking item may include a brief rest, as long as the resident does not sit down. These considerations may assist in completing a thorough assessment in isolation. CMS provides training videos on the SNF QRP Training webpage for instructional purposes.
Facilities can use Section GG data to capture potential changes in function that may require skilled intervention by completing interim assessments. It is the role of the interdisciplinary team to identify potential impacts of isolation on a patient’s biopsychosocial wellbeing and intervene as appropriate.
Finally, review the submission requirements for the SNF-QRP, so a technicality does not overshadow the successful outcomes your teams are creating. Avoid dashes, utilize the activity not attempted codes as necessary, incorporate at least one goal into the patient’s care plan and submit the completed data for at least 80% of your Medicare A claims.
The interdisciplinary team should champion the role of data collection, even in a pandemic, to ensure that we are facilitating the appropriate plan of care, capturing the true picture of the resident’s needs and maintaining the highest quality of rehabilitation and care. Our patients are counting on us!
CMS reports a new issue is affecting some inpatient hospital and skilled nursing facility (SNF) claims when an interrupted stay is billed at the end of the month. The system incorrectly assigns edits U5601-U5608 (overlapping a hospital claim).
If you billed the interrupted stay correctly, and your claim is rejected, modify your billing so the claim spans past the last day of the interrupted stay:
Bill two months at a time, or
Bill a month plus the days in the following month that span the interrupted stay plus 1 day
According to CMS, adjusting the statement covered from and through dates to encompass the entire interrupted stay will allow your claim to process and pay correctly. Medicare Administrative Contractors will finalize any suspended claims that meet the criteria, so you can make corrections and resubmit your claim.
If CMS rejected an inpatient hospital claim, the hospital should ask the SNF to modify their claim. Until October 5, a SNF cannot submit an adjustment to a paid claim; they must cancel the paid claim and all subsequent claims in the same stay and resubmit them in sequential order.
External reviewers have begun targeting Section GG as a focal point of pre/post-pay medical review audits. Because the PDPM function score is derived from Section GG data, and that score correlates to a case mix group for payment, reviewers will seek supportive documentation for decision making related to coding on the MDS.
Therapy evaluations, recertifications, and discharge documents serve as clinical support of that decision making.
Section GG coding should be reflective of the patient’s clinical characteristics.
Objective data within the therapy evaluation/discharge should correlate to the section GG scores.
Example: Bathing noted as Min assist by OT would be scored as 3 – Partial/Moderate Assistance.
Ensuring accurate data information at the beginning of the stay is the first key to successful outcomes. Accurate coding on sections I, C, and K of the MDS are critical. This clinical classification serves as a predictor of resource needs (therapy needs) from CMS and establishes an admission (baseline) for the patient that may be used as parameters in the future for patient progression.
Consider implementing proactive internal audits that review supportive documentation for MDS coding and continue to educate staff on proper coding to strengthen medical review success.
To access our tools for success, please CLICK HERE.
The U.S. Department of Health and Human Services (HHS) has provided more detailed Provider Relief Fund (PRF) reporting guidance. HHS reports they will be releasing more detailed reporting instructions by August 17, 2020.
These reporting instructions will provide directions on reporting obligations applicable to any provider that received a payment from the following CARES Act/PRF distributions:
General Distributions:
Initial Medicare Distribution
Additional Medicare Distribution
Medicaid, Dental & CHIP Distribution
Targeted Distributions:
High Impact Area Distribution
Rural Distribution
Skilled Nursing Facilities Distribution
Indian Health Service Distribution
Safety Net Hospital Distribution
According to HHS, the reporting system will become available to recipients for reporting on October 1, 2020.
All recipients must report within 45 days of the end of CY 2020 on their expenditures through the period ending December 31, 2020.
Recipients who have expended funds in full prior to December 31, 2020 may submit a single final report at any time during the window that begins October 1, 2020, but no later than February 15, 2021.
Recipients with funds unexpended after December 31, 2020, must submit a second and final report no later than July 31, 2021.
Detailed PRF reporting instructions and a data collection template with the necessary data elements will be available through the HRSA website by August 17, 2020.
Several new Centers for Medicare & Medicaid Services (CMS) initiatives designed to protect nursing home residents from COVID-19 have been announced. Read Reliant’s Real Time Memo covering the new funding, enhanced testing, and additional technical assistance and support from CMS.
The Centers for Medicare & Medicaid Services (CMS) announced they will provide a targeted approach for additional resources to nursing homes in COVID-19 hotspot areas.
CMS reports that plans include the following:
Deployment of Quality Improvement Organizations (QIOs) to nursing homes in the hotspot areas.
Implementation of an enhanced survey process tailored to meet the specific concerns of hotspot areas.
Coordination of federal, state and local efforts to leverage all available resources to these facilities.
CMS reports the purpose of these efforts is to target facilities with known infection control issues by providing resources and support that will help them improve quality and safety and protect vulnerable Americans.
In the July 17th MLN Matters Special Edition Article, Medicare Fee-for Service (FFS) Response to the Public Health Emergency on the Coronavirus (COVID-19), CMS provided updates on both diagnostic testing and SNF benefit period waiver.
Medicare Coverage of COVID-19 Testing for Nursing Home Residents and Patients
CMS instructed Medicare Administrative Contractors and notified Medicare Advantage plans to cover coronavirus disease 2019 (COVID-19) laboratory tests for nursing home residents and patients.
Starting on July 6, 2020, and for the duration of the public health emergency, consistent with sections listed in the CDC guidelines titled, “Interim SARS-CoV-2 Testing Guidelines for Nursing Home Residents and Healthcare Personnel,” original Medicare and Medicare Advantage plans cover diagnostic COVID-19 lab tests.
Diagnostic Testing
Testing residents with signs or symptoms of COVID-19
Testing asymptomatic residents with known or suspected exposure to an individual infected with SARS-CoV-2, including close and expanded contacts (e.g., there is an outbreak in the facility)
Initial (baseline) testing of asymptomatic residents without known or suspected exposure to an individual infected with SARS-CoV-2 as part of the recommended reopening process
Testing to determine resolution of infection
Original Medicare and Medicare Advantage Plans don’t cover non-diagnostic tests.
Skilled Nursing Facility (SNF) Benefit Period Waiver – Provider Information
In the MLN Medicare Fee-For-Service (FFS) Response to the Public Health Emergency on the Coronavirus (COVID-19) article, CMS provided clarification in three areas on the SNF Benefit period waiver:
The waiver authorizes a one-time renewal of benefits for an additional 100 days of Part A SNF coverage without first having to start a new benefit period (this waiver will apply only for those beneficiaries who have been delayed or prevented by the emergency itself from commencing or completing the process of ending their current benefit period and renewing their SNF benefits that would have occurred under normal circumstances).
Beneficiaries who exhaust their SNF benefits can receive a renewal of SNF benefits under the waiver except in one particular scenario: that is, those beneficiaries who are receiving ongoing skilled care in a SNF that is unrelated to the emergency, as discussed in the article.
To bill for the benefit period waiver: submit a final discharge claim on day 101 with patient status 01, discharge to home and readmit the beneficiary to start the benefit period waiver.
Shipping of testing supplies was initiated the week of July 20th and will continue over the following 14 weeks.
Testing distribution is being prioritized based on epidemiological hotspot data.
Facilities must have a Clinical Laboratory Improvement Amendments (CLIA) Certificate of Waiver in order to receive the testing equipment.
CMS reports they will expedite review of CLIA waivers for COVID-19 testing.
For more information on how to obtain a CLIA waiver, CLICK HERE.
To be eligible, in addition to having a current CLIA Certificate of Waiver, the nursing home must meet certain epidemiological criteria.
For the list of nursing homes receiving instruments and tests in the first wave, CLICK HERE.
Testing Information
Each facility will receive at least one diagnostic test instrument (from manufacturers QUIDEL or BD) and approximately 400 tests to get started (these numbers will be adjusted for the size of the facility).
Additional antigen tests can be ordered at $25/test through a concierge service from the respective manufacturer.
The test instruments have the capacity to perform 15-20 antigen tests within an hour with near immediate results.
CMS indicated the Medicare program does not reimburse for surveillance testing, but if a patient tests positive, the test may be billed as diagnostic.
Facilities were encouraged to work with other facilities or to potentially share equipment until supply needs for each facility can be met.
CMS reported that they are aware of the likelihood of false negatives with rapid testing; however, the quick result can prove beneficial to the facility for infection control compared to the current lag time of results from the lab.
Additionally, on-site rapid testing may prove beneficial not only due to results obtained more quickly, but it is also more cost effective (the cost of on-site tests is $25 as opposed to the $100-$150 per test cost for current laboratory tests).
For CMS’ FAQ document regarding COVID-19 testing platforms and tests, CLICK HERE.
To access the press release from HHS regarding testing, CLICK HERE.
Sandra Douglas was transferred to Riverfront Rehabilitation for therapy needs following a right sided CVA. Upon admission, Mrs. Douglas was evaluated by and participated in skilled PT, OT, and SLP where she worked on improving independence in many areas including mobility, ADLs, communication, and swallowing.
Progress in therapy took a couple of detours when Sandra tested positive for COVID-19 and had a hospital stay for pneumonia. This setback didn’t stop Sandra or her therapists!
Sandra worked very hard in all areas of therapy especially communication and swallowing. At the beginning of her stay, she was nonverbal and received nutrition exclusively through her PEG tube. As her communication improved, she began asking for her grandson and daughter. The therapy staff was able to help Sandra communicate with them by phone and Facetime.
On the last day of therapy, Sandra was able to verbalize to her SLP that she was hungry. Due to the significant progress made with her swallowing ability, she was able to enjoy chips and soda!
Sandra was able to safely discharge home with her grandson and daughter. According to the therapy staff, Sandra is a true testament of how hard work pays off.
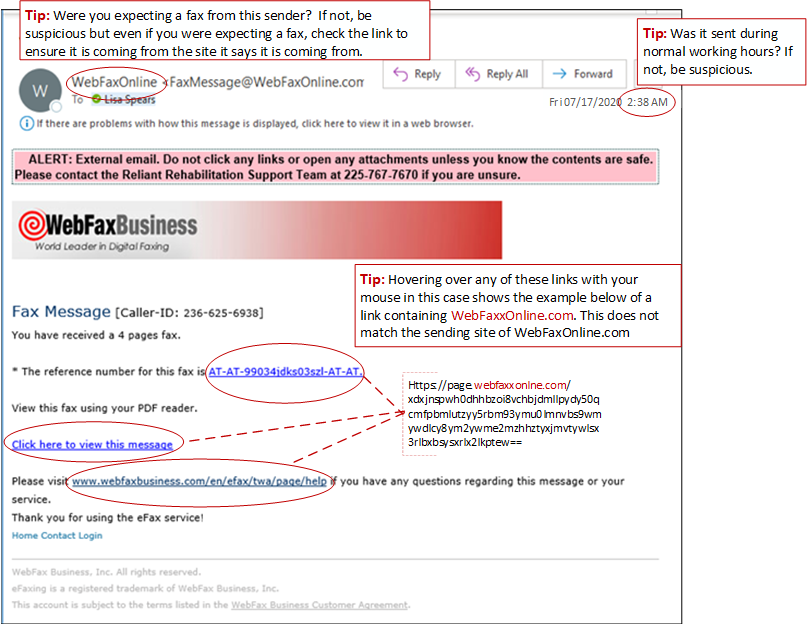
Alexander Bain invented the “Electric Printing Telegraph” in 1843 which became the world’s first faxing device. One hundred seventy-seven years later, we still use fax, and so do hackers. Faxing is so commonly used in our industry that we sometimes forget to be cautious. Hackers use it to send phishing emails which entice users to click on links that download malicious codes. In some instances, you are required to enter your credentials, giving the hacker the opportunity to steal them.
To avoid becoming a victim of fax phishing, see the example email below with tips to stay safe.