
| Phishing attacks are non-stop year-round, and attackers take advantage of holidays and other seasonal events, like tax time, to trick you into clicking links to provide User IDs and passwords. When a phishing attempt is successful, the “Bad Actor” obtains your email login information, and can use your email account to obtain data. Do you have resident information such as face sheets in your emails? If so, there is a wealth of PHI that criminals can use to commit fraud and identity theft. Stay vigilant with these tips. |
PDPM Part 5: Quantity to Quality: PDPM Assessment Schedule
Over the years, the burden associated with the current Medicare required assessment schedule has become “just part of the job.” Staffing of the MDS office is largely driven by Medicare part A census because all residents admitting to a facility for a skilled part A stay will receive a 5-day assessment and depending upon their length of stay may also have a 14-day, 30-day, 60-day, and 90-day assessment. Changes in therapy delivery trigger an additional set of required assessments.
CMS has boasted The Patient Driven Payment Model (PDPM) will reduce provider burden by implementing a significantly reduced required assessment schedule outlined as:5-day Scheduled PPS Assessment | Completed days 1-8 | Covers payment for ALL Part A daysPPS Discharge Assessment | Set as Medicare A stay end date. | Does not affect payment.
In addition to all OBRA requirements remaining the same, the Medicare required PPS assessment schedule consists of these two assessments. That’s it. CMS does acknowledge that changes in the resident’s clinical condition may affect resource use; therefore, they have created an optional Medicare assessment: Interim Payment Assessment (IPA) | Date facility chooses | Payment begins same day as ARD.(triggering event)
Read more about the importance of quality in our MDS assessments here.
Patient Driven Payment Model (PDPM) Frequently Asked Questions
CMS provides a Patient Driven Payment Model (PDPM) web page which houses a variety of resources (comorbidity mapping tools), fact sheets, and a training presentation. An additional resource is the 37 page PDPM Frequently Asked Questions document.
This document covers 14 PDPM topics and answers 92 questions as of 1/28/2019. On the December provider call, stakeholders requested revision dates be provided for reviewers to identify the most recent document update and CMS indicated this would be implemented.
As we progress toward PDPM’s implementation date, be sure to reference CMS’ website frequently to ensure up to date information and clarification.
HIPAA Requirements for Consent to Take and Use Photos and/or Videos

Sharing patient success stories inspires clinicians and other patients alike. It’s vital to ensure the proper policy for sharing that information is followed.
We have provided you with a reference for these HIPAA requirements and Reliant’s Photo Release Form.
Targeted Prove and Educate Trends

As we move into 2019, our focus is honed on the new payment model going into effect in October, PDPM. However, CMS continues to review current trends and initiate audits without a break in sight. With the continuation of Targeted Probe and Education (TPE) audits on the rise, strong supporting documentation, accurate billing practices and managing patient stays appropriately must be the focus of our treatment each and every day.
Read article here .
CMS Chief Indicates New Set of Quality Measures in the Future
This week, Baltimore hosted CMS’ Quality Conference. McKnight’s Long Term Care News featured a recap of CMS administrator, Seema Verma’s “fiery speech” in which she indicated the Patient Driven Payment Model is the first step to move SNFs toward an “outcomes-based system.” She acknowledged continued focus on meaningful measures and offered insight into the future for CMS’s new app eMedicare and quality measure ratings.
Read full McKnight’s article .
Draft of the 2019 MDS Item Sets Posted
A new DRAFT version of the 2019 MDS item sets (v1.17.0) , which is scheduled to take effect on October 1, 2019, was posted earlier this month to the MDS technical information webpage .
The files are located in the Downloads section at the bottom of the webpage (see MDS 3.0 Item Sets v1.17.0 (DRAFT) for October 1, 2019 Release [ZIP, 3MB] ).
This early draft is promising of more information to come. Reliant is monitoring CMS’ updates and postings for more information regarding October 2019 MDS and RAI changes.
New Medicare Card Mailing Complete
CMS has finished mailing the new Medicare cards to beneficiaries across the United States.
CMS states Medicare fee-for-service health care providers submitted 58% of claims with new Medicare Beneficiary Identifiers (MBIs) indicating some success with integration. They encourage providers to utilize the new MBIs for all Medicare transactions even though the former Social Security Number-based health insurance claim numbers are permissible during the transition period.
Old cards may be used through December 2019. If a Medicare beneficiary states they have not yet received a new card, instructions are providedhere .
HIPAA Privacy Rule Refresher
Refresh your memory with some of the Privacy Rule points below.
• HIPAA’s Privacy Rule goal is to protect the confidentiality of patient/resident healthcare information.
• Protected Health Information (PHI) is individually identifiable health information collected from an individual and created or received by a health care provider, health plan, or health care clearing house relating to past, present, or future physical or mental health conditions of an individual.
• Information is “individually identifiable” when any one or more of 18 types of identifiers can be used to identify an individual (e.g. name, address, dates such as birth date, account number etc.)
• The HIPAA Privacy Rule applies to healthcare organizations, healthcare plans, healthcare clearinghouses, and Business Associates with access to Protected Health Information (PHI).
• PHI can be in paper form, electronic as well as in verbal communications.
• Photos and videos of patients/residents are PHI and require documented authorization to take and use. • Access to PHI must be restricted to the minimum access needed to accomplish the intended objective.
• PHI cannot be used or disclosed without documented patient authorization unless it is for any of the following purposes or situations:
o Use or disclosure to the patient
o Use or disclosure for treatment, payment, or general healthcare operations
o Use or disclosure if the individual has the opportunity to agree or object to a disclosure such as a patient bringing a family with them when discussing care with a physician
• Covered Entities (CE) are required to provide residents/patients with a Notice of Privacy Practices (NPP) to tell how the CE may use and share their health information.
• Disposal of documents containing PHI must be rendered unreadable. Shredding is the most common method of disposal. Before disposal, be sure to follow your organization’s data retention policies.
For more information regarding HIPAA Privacy, visit www.hhs.gov.
CMS’ Calendar Year 2019 Medicare Physician Fee Schedule Final Rule
On November 1, 2018, the Centers for Medicare & Medicaid Services (CMS) issued a final rule that includes updates to payment policies, payment rates, and quality provisions for services furnished under the Medicare Physician Fee Schedule (PFS) on or after January 1, 2019.
Reliant’s Real Time Memo, which summarizes the final rule, can be downloaded here. The following is included in the summary:
- Conversion factor update
- Discontinuation of functional status reporting (G-code) requirements for outpatient
- Update on outpatient physical therapy and occupational therapy services furnished by assistants
- KX modifier attestation amount
- Medicare telehealth services update
Payment provisions
Nursing Facility Case-Mix Payment Changes October 1, 2019
CMS issued an informational bulletin earlier this month notifying providers of changes that will impact states’ payments for Medicaid beneficiaries in the nursing home setting.
The bulletin indicates with the implementation of PDPM in October 2019 a new optional assessment, specific for states that rely on RUG-III and RUG-IV assessment schedule, will be available. The assessment will be active from 10/1/2019 through 9/30/2020, at which time states will have to determine an alternate calculation system for Medicaid payment. Additional detail was provided in the December 11th MLN call. Read full bulletin here.
ICD-10 Updates!
Last month we proceeded with our series which dives into critical elements of PDPM by looking at ICD-10 coding. Due to updates provided by CMS we will take one more look at ICD-10 processes for PDPM.
During the open door forum on 11/29/2018, CMS validated information on the PDPM webpage indicating a new MDS item set will be active on October 1, 2019 which will guide the clinical category mapping for the resident. According to CMS’ training materials, new item set I0020B “What is the main reason this person is being admitted to the SNF?” allows for the primary SNF diagnosis to be entered when the response to I0020 “Indicate the resident’s primary medical condition category” is identified as 01-13. The training also provides detailed information about the new items for recording the patient’s surgical history using J2100-J5000. (As of 11/29/2018 CMS notes an error on the PDPM webpage resource New MDS Items which records I0020 as I0200).
It’s important to recognize that although this new item set replaces 18000A as the primary diagnosis mapping line, the codes entered in I8000 and identified throughout section I still require critical thinking and accuracy to ensure accurate reimbursement as these areas contribute directly to SLP comorbidities and conditions, nursing conditions and the non-therapy ancillary comorbidity score.
SNF Open Door Forum: 11/29/2018
In the last open door forum of the year, CMS provided the following information:
• PDPM Webpage is now active. The site provides CMS created fact sheets, FAQ’s, training presentation, and resources specific to PDPM preparation CMS has created as PDPM specific email for questions or clarification needs.
• SNF VBP updates included clarification that providers incentive multipliers are available via CASPER reports. Phase I correction request review is currently in progress. Reconciled corrections will be updated via reports in the CASPER system. The Medicare Administrative Contractor (MAC) will directly apply the incentive percentage when making payment. More information is available on the SNF VBP webpage.
• SNF QRP data now posted on Nursing Home Compare. The next refresh will be in late January. Providers will receive preview reports 30 days prior. CMS directs any questions to the SNF QRP help desk.
• CMS indicated SNF QRP edit 3907 for discharge goal coding will be retired due to stakeholder feedback regarding its relevance; however, edit 3891, warning for discharge coding, will continue.
• CMS reiterated the resources available through the Civil Money Penalty Reinvestment Program (CMPRP). CMPRP is a three-year effort to reduce adverse events, improve staffing quality and improve dementia care in nursing homes.
Hurricane Michael and Medicare Disaster Related Florida and Georgia Claims
CMS provided a revised MLN Matters article addressing providers in the states of Florida and Georgia who were affected by Hurricane Michael. Read full article here .
The Department of Health and Human Services provides healthcare emergency preparedness information via the Assistant Secretary for Preparedness and Response (ASPR) website .
Updated Rankings Available for SNFs Participating in Value Based Purchasing Program
CMS is providing updated rankings for all SNFs included in the Fiscal Year (FY) 2019 VBP program year.
A list of each SNF’s incentive payment multiplier and updated ranking can be found on the SNF VBP website . The incentive payment multiplier applicable to each SNF is unchanged from the multiplier that CMS previously included in the SNF’s FY 2019 Annual Performance Score Report.That multiplier will be used to adjust the federal per diem rate otherwise applicable to the SNF for services furnished from October 1, 2018 through September 30, 2019.
Keep Information Safe with Good Password Practices
These days we’re all overloaded with the number of accounts that require credentials and remembering them is impossible. Using the same password for different accounts is tempting—like having one handy key that opens every lock you use. But reusing passwords is not the solution.
Compromised passwords are one of the leading causes of data breaches, and reusing passwords can increase the damage done by what would otherwise be a relatively small incident. Cybercriminals know that people reuse credentials and often test compromised passwords on commonly used sites in order to expand the number of accounts they can access.
For instance, if you use the same password for your work email as for Amazon or your gym membership, a breach at one of those companies puts your work emails at risk. Reusing credentials is like giving away copies of the key that opens all your locks. Before reusing a password for different accounts, especially across work and personal ones, think of all the data that someone could get into if they got that credential.
Here are some tips to help you avoid falling in this trap:
• Use completely separate passwords for work and personal accounts.
• Avoid words that can easily be guessed by attackers, like “password” or “September2017,” or predictable keyboard combinations like “1234567,” “qwerty,” or “1q2w3e4r5t.”
• Add some complexity with capitalization or special characters if required. “Fido!sAnAwesomeDog” is a stronger password than your pet’s name.
• Just adding numbers or special characters at the end of a word doesn’t increase security much, because they’re easy for software to guess.
• Avoid words like your kids’ names that could easily be guessed by coworkers or revealed by a few minutes of online research.
• Answers to security questions are often easily found— your mother’s maiden name is public record—so pick another word for whenever that question comes up.
SNF QRP Data on Nursing Home Compare as of 10/24/2018
CMS has added five SNF QRP measures to Nursing Home Compare.
Download the CMS’ Fact Sheet.
Visit Nursing Home Compare.
SNF Quality Reporting Program Submission Deadline Approaching
The deadline for the Skilled Nursing Facility (SNF) Quality Reporting Program MDS data submission for April 1, 2018-June 30, 2018 (2nd quarter) is November 15, 2018.
Review resources:
Current data collection (2018 4th quarter) includes new section GG items added on October 1, 2018. Download Reliant’s resource here .CMS recommends that providers run applicable validation/analysis reports prior to each quarterly reporting deadline in order to ensure all required data has been submitted.
CMS Released Proposed Rule to Promote Program Efficiency
On September 20, 2018 CMS released a proposed rule titled “Regulatory Provisions to Promote Program Efficiency, Transparency, and Burden Reduction”. AHCA notes this proposed rule impacts regulations for 12 different types of healthcare providers and suppliers impacted by CMS requirements for emergency preparedness and hospice.
Comments are open through November 19, 2018. View proposed rule here.
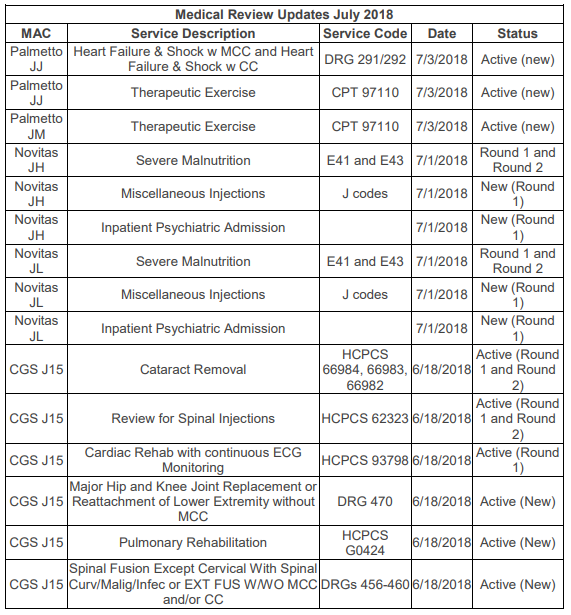
Clinical Appeals Corner: Therapeutic Exercise Added to TPE Medical Reviews
Medicare Administrative Contractors (MACs) Palmetto (Jurisdictions J and M), Novitas (JH and JL), and CGS (J15) have each added new issues for their Targeted Probe and Educate (TPE) medical reviews. You can see all of these additions in the table at the end of this article. One new addition for Palmetto JJ and JM Part A (hospitals) is the review of outpatient therapeutic exercise, CPT code 97110. Palmetto does not include details of exactly what they will be looking for in this audit, but as noted above, rehabilitative therapy services have long been the subject of Medicare reviews. Several recently updated articles on the website of another MAC, Wisconsin Physician Services (WPS), identify some of the major concerns traditionally seen with therapy services.
Plan of Care Certification
According to a WPS article from the Comprehensive Error Rate Testing (CERT) A/B MAC Outreach & Education Task Force, “The leading cause of payment errors for therapy services is “insufficient” documentation in the medical records. Documentation is often missing the required elements as outlined in the CMS Internet-Only Manual (IOM) Publication 100-02, Chapter 15, Sections 220 and 230.” Specifically, the plan of care is often missing a legible, dated physician or non-physician practitioner (NPP) signature for certifying the plan of care (POC).
Certification by the physician or NPP certifies that individual needed therapy services are being provided under a POC established by a physician/NPP or by the therapist providing such services and periodically reviewed by a physician/NPP while the individual is or was under the care of a physician. Certification is required for coverage and payment of a therapy claim. Certification requires a dated signature on the plan of care or some other document that indicates approval of the plan of care. In addition to the physician/NPP’s signature, the legible signature and professional identity of the individual who established the plan, as well as the date it was established, must be recorded with the plan.
Required elements of the plan of care include:
• Diagnoses (both medical diagnosis and patient’s functional limitations);
• Long term treatment goals that are measurable and pertain to the identified functional impairments; and
• Type, amount, duration and frequency of therapy services.
Documentation of Time
Medicare requires that the daily treatment note include total timed code treatment minutes and total treatment time in minutes. Most CPT codes used for therapy services specify the direct (one-on-one) time spent with the patient in per 15-minute intervals. This means the number of billable units for these codes is based on time. When more than one service represented by 15-minute timed codes is performed in a single day, the total number of minutes of all timed services determine the number of timed units billed. The minutes for all timed codes must be summed to determine the appropriate units to bill. Consider only the time actually spent in the delivery of the therapy service or modality. Pre- and post-delivery services are not to be counted in determining the treatment service time. This WPS article includes a chart of the number of units based on the minutes spent treating the patient and several examples of appropriate billing.
Services described by untimed therapy codes are reported as 1 unit. The time spent for these untimed services should also be documented and summed with the timed code minutes to report the total Reliant Rehabilitation Proprietary Information treatment time in minutes. However, do not include the minutes of untimed codes to determine the units of service to bill.
In addition to timed code treatment minutes and total treatment time minutes, the daily treatment notes should include:
• Date of treatment.
• Identification of each specific intervention/modality provided and billed (both timed and untimed codes).
• Signature and professional identification of the qualified professional who furnished the services; or, for incident to services, supervised the services, including a list of each person who contributed to the treatment.
Medical Necessity
Not as objective as the presence of a signature or the number of minutes, but equally important is documentation to support that therapy services are medically necessary and require the skills of a therapist. This is where the story told by the therapists in the evaluation, plan, progress notes, and treatment notes comes together to justify the need for therapy services.
Ask yourself if your documentation sufficiently addresses the following questions:
• Did the patient experience a significant decline in function that requires therapy?
• Would the patient have been able to recover function without therapy?
• Does the documentation include specific, objective measures of the patient’s prior level of function, current level of function, and expected level of function?
• Are the type, frequency, and duration of therapy services appropriate based on acceptable standards of medical practice and the patient’s condition and potential for improvement?
• Is the patient improving or regression prevented due to the therapy treatments?
• Has the patient reached maximum potential?
• Could therapy services or additional therapy services be safely and effectively furnished by nonskilled personnel?
One last WPS article that contains good information for therapy services can be found here.
Re-evaluations
Re-evaluations are not routine, recurring services and are covered only if the documentation supports the need for further tests and measurements after the initial evaluation. Re-evals are appropriate when:
• There are new clinical findings,
• There is a significant change in the patient’s condition, or
• The patient fails to respond to the therapeutic interventions outlined in the plan of care.
With all the attention over the years on therapy services documentation, hopefully your facility’s therapy documentation meets all of Medicare’s requirements and supports the need for skilled therapy services. It will be interesting to see what Palmetto finds on their TPE reviews.
Debbie Rubio, BS, MT (ASCP), is the Manager of Regulatory Affairs and Compliance at Medical Management Plus, Inc. Reliant Rehabilitation Proprietary Information