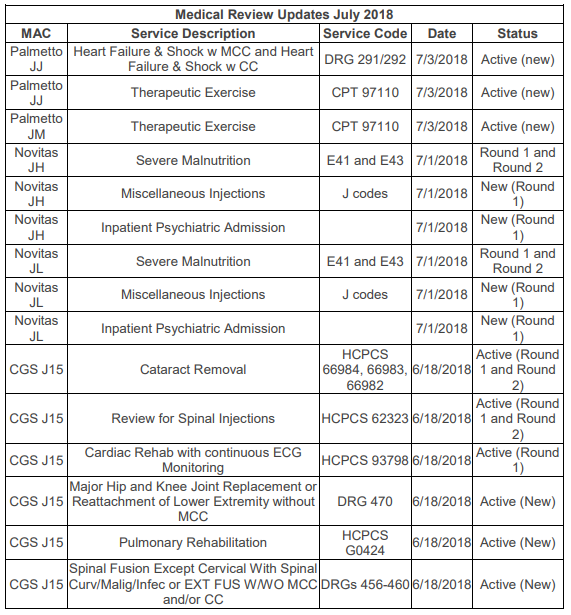
Medicare Administrative Contractors (MACs) Palmetto (Jurisdictions J and M), Novitas (JH and JL), and CGS (J15) have each added new issues for their Targeted Probe and Educate (TPE) medical reviews. You can see all of these additions in the table at the end of this article. One new addition for Palmetto JJ and JM Part A (hospitals) is the review of outpatient therapeutic exercise, CPT code 97110. Palmetto does not include details of exactly what they will be looking for in this audit, but as noted above, rehabilitative therapy services have long been the subject of Medicare reviews. Several recently updated articles on the website of another MAC, Wisconsin Physician Services (WPS), identify some of the major concerns traditionally seen with therapy services.
Plan of Care Certification
According to a WPS article from the Comprehensive Error Rate Testing (CERT) A/B MAC Outreach & Education Task Force, “The leading cause of payment errors for therapy services is “insufficient” documentation in the medical records. Documentation is often missing the required elements as outlined in the CMS Internet-Only Manual (IOM) Publication 100-02, Chapter 15, Sections 220 and 230.” Specifically, the plan of care is often missing a legible, dated physician or non-physician practitioner (NPP) signature for certifying the plan of care (POC).
Certification by the physician or NPP certifies that individual needed therapy services are being provided under a POC established by a physician/NPP or by the therapist providing such services and periodically reviewed by a physician/NPP while the individual is or was under the care of a physician. Certification is required for coverage and payment of a therapy claim. Certification requires a dated signature on the plan of care or some other document that indicates approval of the plan of care. In addition to the physician/NPP’s signature, the legible signature and professional identity of the individual who established the plan, as well as the date it was established, must be recorded with the plan.
Required elements of the plan of care include:
• Diagnoses (both medical diagnosis and patient’s functional limitations);
• Long term treatment goals that are measurable and pertain to the identified functional impairments; and
• Type, amount, duration and frequency of therapy services.
Documentation of Time
Medicare requires that the daily treatment note include total timed code treatment minutes and total treatment time in minutes. Most CPT codes used for therapy services specify the direct (one-on-one) time spent with the patient in per 15-minute intervals. This means the number of billable units for these codes is based on time. When more than one service represented by 15-minute timed codes is performed in a single day, the total number of minutes of all timed services determine the number of timed units billed. The minutes for all timed codes must be summed to determine the appropriate units to bill. Consider only the time actually spent in the delivery of the therapy service or modality. Pre- and post-delivery services are not to be counted in determining the treatment service time. This WPS article includes a chart of the number of units based on the minutes spent treating the patient and several examples of appropriate billing.
Services described by untimed therapy codes are reported as 1 unit. The time spent for these untimed services should also be documented and summed with the timed code minutes to report the total Reliant Rehabilitation Proprietary Information treatment time in minutes. However, do not include the minutes of untimed codes to determine the units of service to bill.
In addition to timed code treatment minutes and total treatment time minutes, the daily treatment notes should include:
• Date of treatment.
• Identification of each specific intervention/modality provided and billed (both timed and untimed codes).
• Signature and professional identification of the qualified professional who furnished the services; or, for incident to services, supervised the services, including a list of each person who contributed to the treatment.
Medical Necessity
Not as objective as the presence of a signature or the number of minutes, but equally important is documentation to support that therapy services are medically necessary and require the skills of a therapist. This is where the story told by the therapists in the evaluation, plan, progress notes, and treatment notes comes together to justify the need for therapy services.
Ask yourself if your documentation sufficiently addresses the following questions:
• Did the patient experience a significant decline in function that requires therapy?
• Would the patient have been able to recover function without therapy?
• Does the documentation include specific, objective measures of the patient’s prior level of function, current level of function, and expected level of function?
• Are the type, frequency, and duration of therapy services appropriate based on acceptable standards of medical practice and the patient’s condition and potential for improvement?
• Is the patient improving or regression prevented due to the therapy treatments?
• Has the patient reached maximum potential?
• Could therapy services or additional therapy services be safely and effectively furnished by nonskilled personnel?
One last WPS article that contains good information for therapy services can be found here.
Re-evaluations
Re-evaluations are not routine, recurring services and are covered only if the documentation supports the need for further tests and measurements after the initial evaluation. Re-evals are appropriate when:
• There are new clinical findings,
• There is a significant change in the patient’s condition, or
• The patient fails to respond to the therapeutic interventions outlined in the plan of care.
With all the attention over the years on therapy services documentation, hopefully your facility’s therapy documentation meets all of Medicare’s requirements and supports the need for skilled therapy services. It will be interesting to see what Palmetto finds on their TPE reviews.
Debbie Rubio, BS, MT (ASCP), is the Manager of Regulatory Affairs and Compliance at Medical Management Plus, Inc. Reliant Rehabilitation Proprietary Information